Objectives: To review the incidence, clinical presentation, and management of meningeal hemangiopericytomas of the lateral skull base and cerebellopontine angle (CPA), and describe a case of anaplastic hemangiopericytoma of the CPA and middle cranial fossa presenting as a middle ear mass.
Study Design: Case report and literature review
Methods: The case of a patient with hearing loss and a middle ear mass, ultimately found to have invasive, anaplastic hemangiopericytoma of the skull base, is presented. The clinical, radiologic, and pathologic features of hemangiopericytomas are discussed. The trans-zygomatic approach for excision of lesions in the middle cranial fossa is described.
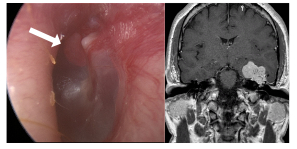
Results: A 51-year-old male presented to a tertiary center with a one year history of progressive, unilateral hearing loss, pulsatile tinnitus, mild disequilibrium, and word finding difficulty. Physical examination demonstrated a vascular mass in the left middle ear abutting the tympanic membrane. Magnetic resonance imaging revealed a 4 cm, T1-/T2-isointense, contrast-enhancing mass with a dural tail centered over the left petrous bone in the middle cranial fossa. The mass was eroding the middle fossa bone and extending into the middle ear, and the surrounding temporal lobe tissues exhibited extensive edema. A trans-zygomatic approach with a pterional craniotomy was used to access the middle cranial fossa, exposing a well-encapsulated, highly vascular mass extending into the temporal lobe. Manipulation of the tumor resulted in significant hemorrhage, raising the possibility that the mass was not a typical meningioma. After removing the mass from the temporal lobe, middle ear, and Eustachian tube, an anterior petrosectomy was performed to remove tumor from the internal auditory canal (IAC) and carotid artery region. The facial nerve near the IAC was completely encased in tumor, and all but a small amount of tumor firmly adherent to the nerve was successfully removed. The final pathologic diagnosis was anaplastic hemangiopericytoma (WHO Grade III). Metastatic workup revealed no extracranial disease, and the patient underwent adjuvant radiation therapy. He continues to do well with only mild disequilibrium and anomic aphasia at six-month follow-up.
Conclusions: Hemangiopericytomas are rare, malignant neoplasms that are aggressive and highly vascular in nature. Current management recommendations include mass excision followed by radiotherapy. Continued close surveillance is required for patients with anaplastic hemangiopericytoma due to the aggressive nature of this tumor and its propensity for recurrence or metastasis.