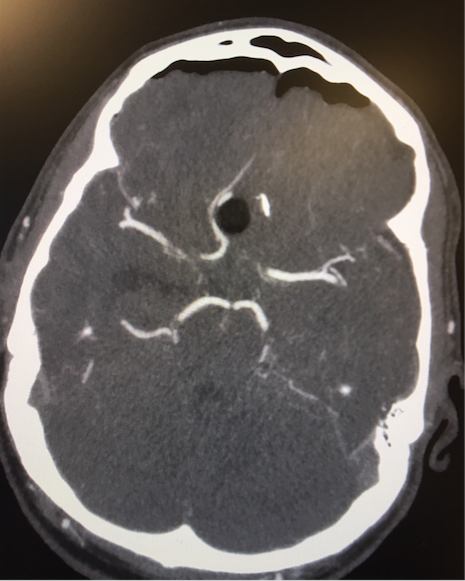
We report the unusual case of a 35 year old man who presented post self-insertion of a foreign body (a toothbrush with the bristled end snapped off) trans-nasally whilst suffering from a drug-induced psychosis. The tip of the retained object extended intracranially as far as the right foramen of Munro and caused unilateral obstructive hydrocephalus requiring emergency external ventricular drain insertion. There was no evidence of significant intracranial haemorrhage on initial imaging but the post-communicating segments of both anterior cerebral arteries were significantly displaced by the object. After deliberating the safest surgical approach, we elected to perform a bifrontal craniotomy to approach the anterior fossa floor inter-hemispherically, in order to gain proximal control of the anterior cerebral arteries and protect them from laceration. Once this was achieved, the foreign body was removed transnasally by the ENT surgeon, who had performed prior ligation of the ipsilateral anterior ethmoidal artery to prevent catastrophic nasal haemorrhage. Nasoendoscopy revealed surprisingly little damage to the nasal cavity. The skull base defect was repaired utilizing split calvarial bone graft obtained during the craniotomy, and a vascularized pericranial flap. Postoperatively the patient did not develop a CSF leak and displayed no signs of meningitis. His psychosis self-resolved within two weeks post-operatively and he was discharged home after a 2-week course of intravenous antibiotics and with psychiatry input. A delayed post-operative MRI demonstrated no obvious abscess, empyema or cerebral infarction. On review of the literature, such extreme cases of skull base penetrating injury appear to be rare and there is little technical advice available on optimal surgical strategies. This case provides an opportunity to discuss the management of such injuries and adds to a currently scarce body of knowledge on the topic.